


You had a higher relative risk of dying with Covid in 2021 than 2020
Despite the vaccines, lockdowns, and mandates. This is what the CDC data shows.

My fellow Americans: how was your 2021, Covid year II? Did you know that despite the vaccines and lockdowns, the masks and mandates, the Fauci-worship and the media censorship – despite all this, you had a higher relative risk of dying with Covid in 2021 than in 2020? This is what the CDC data shows. (Yes, really. Verifiably).
The prime exception, perversely enough, being people in the Age Range of 85 years and older. We’ll call Age Range 75-84 a push.

We will take 2020, Covid Year I, as our “control group” in this natural experiment. Remember, in 2020: no vaccines were widely available – and so no vaccine rollouts or mandates. Blue states were not yet completely sold on lockdowns and the like, and Donald Trump was still President. So 2021, Covid Year II, will serve as our treatment group: vaccines, lockdowns, mandates, Anthony Fauci given free reign, and Joseph Biden as our President.
Relative risk here means the risk you faced in 2021 compared with the risk you faced in 2020. I will explain shortly below how that is determined: but this is a fundamental tool in Biostatistics, something a student would likely learn their first year as a undergraduate. So nothing truly exotic or mysterious.
Besides using a fundamental and widely accepted method for comparison, do you know what else matters? Transparency – and reproducible results, openness and sharing. So in that spirit;
First, let me provide you with a direct link to the original CDC data source: Provisional Death Counts for COVID-19. (Accessed for this report on 19 January 2022).
Second, in the interests of full transparency – Open Science, Open Source – let me share the link to the Github repository with code and data used to generate the visualizations and summary statistics below: Covid2021vs2020.
Third, let me provide you with a link to an arguably prettier, more interactive version of these results. More “just the facts” – just the data: Covid in the USA: 2021 vs. 2020.
The findings I present below are as objectively correct, as factual, as the CDC data permits. (Read their disclaimer, please). So go ahead. Check the data. Try to reproduce my results. I insist.
So one more time, bottom line up front:
If you were under the age of 75, you had a higher relative risk of dying with Covid in 2021 than you did in 2020.
This despite everything (or perhaps in part because of it?): the vaccine rollout and mandates, the lockdowns and restrictions, et cetera.
Btw, why use “dying with Covid” as opposed to “dying from Covid” – one might ask? Because I am working with the CDC data, and the CDC collects data on people who died with Covid. They have estimated that roughly 90% of the people who “died with Covid” also “died from Covid”: but we might expect that estimate to change considerably over next year.
So again, I am working with the CDC data: “Dying with Covid” is the proper variable for which the observations have been reported.
Let’s look at the data. The CDC data. The USA government provided data. But first I do need to clarify what is meant by relative risk. (If you already know all this jazz, skip down to The Big Picture: All Sexes).

Relative Risk (for those who need a review)
Let’s take two fair dice. The red one has six sides: numbers 1 to 6. The white one has twelve sides: the numbers 1 to 12.
When you pick a number and roll the first die, the red one, you have possible one winning outcome, five possible losing outcomes, and six possible outcomes total. What is your probability of winning? 1 in 6; or 1/6. Now for the second die, the white one, same general deal. Your probability of winning? 1/12.
Which die is risker, the red one or white one? How much risker? The white die with 12 sides, right? Because you only have one way of winning, but eleven ways of losing.
So what is the relative risk of the two dice? How much better is the red die, six sides, compared to the white die, 12 sides? The formula: (1/6) / (1/12). Or, 0.1666667 / 0.08333333. Either way, in this case, the relative risk is 2. You are two times more likely to win with the red die, the six-sided dice, then you are with the white die, the twelve-sided die.
So for the outcome of interest, wining your roll, you doubled your chances with the six-sided red die. Conversely, if you switch among the dice, you cut your chances in 1/2, your relative risk goes to 0.5, with the twelve-sided white die. Not so hard right?
So how do we apply this to biostatistics and public health data? Well, when looking at medical treatments and related interventions, particularly for novel situations, typically we do not know the probabilities in advance. We have to work from the outcomes.
Relative Risk: Simplified Example
Let’s take one typical scenario: a control trial. We will use a greatly simplified example. Here’s a graphic from Wikipedia by Psarka (CC By-SA 4.0), which captures neatly how to calculate the relative risk:
{kind=link}

We have two groups. In the pill group (treatment group), 4/16 had an adverse reaction: so ¼ or 0.25. In the control group, 8/16 had an adverse reaction: so ½ or 0.50. The relative risk ratio: (1/4) / (1/2). Or, 0.25 / 0.50. Which equals ½ or 0.50. So the pill group had ½ the relative risk of having an adverse reaction compared to the control group.
Conversely, the control group had twice the risk of having an adverse reaction: (1/2) / (1/4) or 0.50 / 0.25. Which equals 2. Right? So for our above simplified example, we would say that the pill group had ½ the relative risk of an adverse effect; and the control group had 2 times the relative risk of having an adverse effect.
Relative Risk: CDC Data
So I trust we are good enough to keeping moving. We have an outcome of interest in two different groups. Our outcome of interest: Dying with Covid. As reported in the CDC data for the years 2020 and 2021. Stratified by Age Range and Sex.
We want to know how many people died with Covid / how many people died from all causes.
Wait, you say: the numbers for “how many people died with Covid” are included in “how many people died from all causes.” Yes, correct!
Let’s walk it back to our fair six-sided dice. You picked the number “5”: you have one way of winning, five ways of losing (“1”, ‘2”, “3”, “4”, and “6”), and six total outcomes. Your probability of rolling a “5” is 1/6. Same deal here. “Dying with Covid” is one side of the die, say number “5.” The “Non-Covid Deaths” make up the other sides of die, say numbers “1”, “2”, “3”, “4”, and “6”. The “Dying with Covid” and the “Non-Covid Deaths” make up the “All Causes Death” count.
(If you want to see how the “Dying with Covid” and “Non-Covid Deaths” counts add up to the exact same “All Causes Death” counts as reported by the CDC (19 January 2022), please browse the data table section at our Dashboard).
So if we want to know what was the probability of “Dying with Covid” for 2021, the formula is as follows: “Dying with Covid” / “All Causes Death” for 2021. Good? Call that answer: 2021_probability. Now, if we want to know what was the probability of “Dying with Covid” for 2020, the formula again: “Dying with Covid” / “All Causes Death” for 2020. Call that answer: 2020_probability.
Now, we want the relative risk of Dying with Covid in 2021 compared to 2020. What is the formula? 2021_probability / 2020_probability. Just like the examples we saw earlier: the two dice, and the control trial.
That’s our review of Relative Risk for people who are new to the concept. Again, we have just lived through a natural experiment in history. For our purposes here, 2021 – Covid year II, is our treatment group; 2020 – Covid year I, is our control (the year without vaccines, et cetera). So we must have better results for 2021, for Covid year II. Right?
The Big Picture: All Sexes
Show time, tell time. Ready for some bad news? Well, we do end with some possible good news about Omicron.
Let’s begin with the big picture. The CDC source data is stratified by Age Ranges – this is standard with public health data. It is also stratified by biological sex (Female & Male) – also standard for public health data. We will do a detailed breakdown by biological sex shortly later – some interesting differences emerge. But we will start with the Age Range breakdown per year. (Here comes that graph again).

This graph does NOT show the raw count of deaths per age range: it shows the percentages of Deaths with Covid, and of Non-Covid Deaths. Together, these two make up 100% of Deaths All Causes. (Please note that year 2021 is displayed on top).
Please notice the increased size of the red bars, our outcome of interest, for 2021: we have noteworthy increases in six of the eight Age Ranges. In fact, these are the most densely populated Age Ranges: people 74 years of age and younger! Not good news.
Using Relative Risk, we can bring context to these percentage changes in Death — we can make a controlled, meaningful comparison between 2021 and 2020. 2021, Covid year II: we had vaccines and mandates, ongoing lockdowns and restrictions, et cetera. 2020: no vaccines and hence no vaccine mandates, various lockdowns and restrictions regionally and often partially implemented.
So we should have been doing better in 2021, right? Americans should have had a decreased Relative Risk of Dying with Covid. What do the CDC numbers tell us?
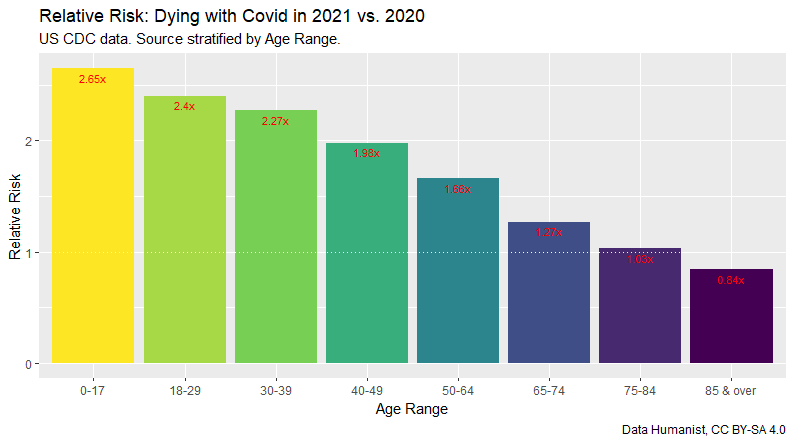
For the Age Ranges 0-17, 18-27, and 30-39, the Relative Risk has more than doubled; for 40-49, nearly so. Disturbing, because these Age Ranges globally so far have had the lowest risk of Covid morbidity.
What this means: if you were between the ages of newly born to 49 years, you had TWICE the relative risk of Dying with Covid in 2021 than in 2020. In other words, and in no uncertain terms, the USA accomplished little to nothing in reducing the relative risk of Covid morbidity.
In no uncertain terms, the USA failed to reduce the relative risk of Covid morbidity for the vast majority of its citizen and residents. In fact, for vast majority of people, relative risk doubled: people were twice as likely to Die with Covid in 2021 than in 2020.
We went backwards not forwards in 2021. That is what data shows. If you would like to look at the raw numbers, please browse the data table section at our Dashboard.
So what is going on in the USA? Let’s break it down further per biological sex. Ladies first.
Ladies first: Biological Females
Although we have progressive activists who deny the reality of biological sex differences, differences in biological sex matter for the purposes of medical research and clinical treatment. Dr. Carolyn M. Mazure, the Norma Weinberg Spungen and Joan Lebson Bildner Professor in Women's Health Research and Professor of Psychiatry and of Psychology at the Yale School of Medicine, offers a nuanced discussion of the same in “What Do We Mean By Sex and Gender?”
I fully endorse Dr. Mazure’s claim that we should no longer understand the terms sex and gender as simply interchangeable. But I also fully endorse Dr. Mazure’s qualification that we have “more than sufficient evidence” proving that “major differences in the biology of women and men” exist, and these differences must not be ignored when developing ways to promote health and treat sickness. Please do read “What Do We Mean By Sex and Gender?”
We have some important differences between the outcomes for biological females versus biological males. Spoiler alert: the outcomes for biological females are worse. I hope this reality will not be ignored because of our current cultural wars.

Similar to All Sexes, we have noteworthy increases the first six Age Ranges. (The increase in Age Range 75-84 is a push: if the Relative Risk hovers close to 1, likely no difference that makes a difference).
As for Age Ranges 75-84, and 85 and older, we should be careful about celebrating these two seeming exceptions.
One possible explanation is an extremely unpleasant one. Our first year of Covid, 2020, with the various nursing home fiascos might well have culled the most vulnerable members of the 85 years and older population. So far, no criminal charges against Andrew Cuomo, former governor of New York; nor against Gretchen Whitmer, governor of Michigan.
The percentages gains in Dying with Covid appear greater for biological females than for all sexes (the earlier graph): they are greater — the relative risk, likewise.

Once again, significant increased risk of Death with Covid across six of the eight Age Ranges. But more disturbing here, for the Age Ranges 0-17, 18-29, and 30-39, the Relative Risk is 2.5 times or greater.
So in 2021, biological females in these age ranges were 2.5 times MORE likely to die with Covid. To express that in percentages: 278%, 256%, and 259% respectively. How are such results an acceptable return on our massive healthcare investment for combatting Covid-19?
The results for biological females are higher than (worse than) the results for all sexes. In regard to Covid (and perhaps other areas), the USA is dropping the ball big-time on women’s health.
Should we be concerned about this? Yes.
But so far, the MSM and the American public health establishment have ignored the Dying with Covid gap as it pertains to biological sex. This may please the Tik-Tok influencers who deny the reality of biological sex differences, but is it in our national best interest?
Brothers in Covid: Biological Males
It is no bromance for the biological males, even if their bad outcomes are slightly better than those of the biological females.

Significant increased risk of Dying with Covid across five of the eight Age Ranges. Age Range 65-74 is close to a push; Age Range 75-84, push; Age Range 85 and older, slight decrease.
Again, we need caution in celebrating even the minor successes at the upper end of the Age Range spectrum. First, we simply have a comparatively smaller population of male adults who are 65 and older. Second, and as mentioned earlier, for 2020 Covid year I, we had an elder care fiasco. Some would argue it amounted to vile criminal misconduct – I am sympathetic to such an argument.
Let’s see the Relative Risk for biological males visualized. You can find the raw numbers in the data table section at our Dashboard.

For the final two Age Ranges, we have results that strongly match with those for the biological females, and which show either a push or slight decrease. Again, we should temper any celebration. But I would be happy indeed to learn that for 2021, we did a much better job protecting our elderly citizens.
Biological Sex Differences(?)
We discussed earlier how for purposes of medical research and clinical treatment, differences in biological sex matter. I also shared and strongly endorse Dr. Carolyn M. Mazure’s vital and nuanced statement, “What Do We Mean By Sex and Gender?”
Let’s compare the Relative Risk results for both biological females and biological males. Visualization below. Raw numbers available in data table section at our Dashboard.

The results clearly indicate that biological females in the Age Ranges from 0-17, 18-29, 30-39, and 40-49 had noticeable increases in relative risk compared to their male cohorts. Period.
Biological females in the Age Ranges from 0-17, 18-29, 30-39, and 40-49 had noticeable increases in relative risk compared to their male cohorts.
Despite (or perhaps in part because of?) everything that year 2021 brought to the table in terms of treatment, biological females died at higher rate in 6 out of 8 age ranges compared to year 2020. (Age Range 75-84 is a push). And again, in five of those Age Ranges, biological females performed noticeably worse than biological males.
Can we discuss this? As a public health matter?
Perhaps we should fully respect people’s rights to gender-identify as they choose, and respect their dignity, and ensure equality of opportunity for all: but as part of that effort, we should also stop denying the reality of biological sex differences.
Conclusion and Speculative Good News
If we made progress on reducing the relative risk of Dying with Covid during 2021, the CDC data does NOT show this. In fact, the opposite. The data shows the relative risk significantly increasing for Age Ranges 0-17, 18-29, and 30-39. These increases seem almost perverse, and out of line with the general global trends as reported thus far. The data also shows the relative risk increasing significantly to moderately for Age Ranges 40-49, and 50-64. Again, a higher relative risk of Dying with Covid is NOT good news.
I will now offer my opinion on the results – the evidence – presented. This is my interpretation.
We Lost Our Way
The USA should have followed the principles outlined in the Great Barrington Declaration, mainly protecting the most vulnerable members of the population while focusing equally on therapeutics as well as vaccination development and promotion.
The Fauci Reign of Error and Terror Must End
The various Fauci-inspired, directed, or recommended mandates, lockdowns, and restrictions were and are vastly counter-productive, deeply destructive, and horrifically wasteful. It may take a generation or more to recover from the economic, social, institutional, and psychological damages brought about by Anthony Fauci’s reign of error and terror.
Omicron is Good News?
Perversely, the good news might be Omicron. It develops poorly — often, not at all — in the lungs. It is primarily an upper respiratory infection generally similar in effects and risk to a common cold. Moreover, and more importantly, many people who have recovered from Omicron seem to have developed robust, polyvariant natural immunity. A safe recovery from Omicron seems to serve as an effective vaccination for the unvaccinated, and a useful booster for the vaccinated. Whereas “science” or rather the technocratic scientism of Fauci et alia has failed us, nature may yet help with providing a partial cure: a means for transforming the Covid pandemic into a mild endemic.
End All Mandates, Phase Out All Restrictions
The global data so far is highly promising albeit not conclusive. But we do know what does NOT work. As pertaining to the general public, it is time to end ALL Covid vaccination mandates, and phase out ALL Covid restrictions.
Thank you for reading.
If you made this far, please share! Also, more data at our Dashboard; and source code available at Github Repo. If you find these resources useful, a cup of coffee would be appreciated.
Data Humanist for American Exile
27 January 2022