


Greater all-cause mortality from the mRNA Covid vaccines versus the old-school adenovirus Covid vaccines? YES, according to one recent study (The Lancet, 5 April 2022).
Concerns about the mRNA vaccines were labelled as either conspiracy theories or irrational fears. It now seems the mRNA evangelists were the ones ignoring the data, practicing faith not science.

If the study by Christine Stabell-Benn, et alia, is confirmed by further research, millions of people were subjected to unnecessary risk. In a vast number of cases, unnecessary risk that was mandated or coerced. As millions of American citizens, to start, were offered a practical choice of only mRNA vaccines: Pfizer or Moderna.
The mRNA vaccines performed differently than their old-school Adenovirus-vector counterparts. We were told “superior,” based on trial data which FDA claimed would take 75 years to release to the public. People trusted or were mandated. Got jabbed.
The count of the mRNA vaccinated expands considerably when we take in the global picture. Moreover, simply because of the law of large numbers, the rigorous and often enforced promotion of mRNA Covid vaccines over their Adenovirus-vector counterparts may well have resulted in tens of thousands of unnecessary deaths.
Please do not say “I knew it all along — I said it all along,” even if you did. This one is bad — rather, potentially horrific. Please do not gloat.
Nothing to celebrate here, if Stabell-Benn, et alia is on the mark — even if we honor their commitment to truth. The researchers set out to study “Beneficial Non-Specific Effects” — the typically positive fallout, the more general health gains, that follow a vaccination campaign. They compared the two vaccine types. Results, an earthquake.

For the above graph and all that follow, lower is better. Lower relative risk. Green shows the mRNA estimate within a 95% Confidence Interval; Blue shows the Adenovirus (old tech) estimate within a 95% Confidence Interval.
(These graphs reproduce the same data in a different format than the Forest graph included in the study. Please also consult the original “Figure 1.” If you are unfamiliar with the term Relative Risk, a brief explanation may be found here).
What are “Beneficial Non-Specific Effects?”
In her interview with UnHerd, Professor Christine Stabell-Benn states an example from a measles vaccination campaign in Africa. At that time, measles accounted for roughly 10% of the deaths in the targeted community.
But after the vaccination campaign was completed, the all-cause mortality rate did not decline by 10% — it declined by over 50%. A benefit over 40+%! How? Why?
Simply, if your immune system was no longer fighting measles, it was free to fight something else. Likewise, the healthier you are, the better your chances — all other things being equal — at coping with various illnesses and life challenges.
So in terms of the all-cause mortality rate, the measles vaccination campaign reaped a 40+% bonus in morality rate decline! It had demonstrable “Beneficial Non-Specific Effects” — health benefits beyond providing protection against the measles, the original disease targeted.
Four Categories of Mortality
Stabell-Benn, et alia, decided to study the “Beneficial Non-Specific Effects” for mRNA and Adenovirus Covid vaccines. They evaluated the performance of each for the following four categories of mortality:
Overall Mortality
Covid-19 Deaths
Cardiovascular Deaths
Other (non-accidental) Deaths
For the study’s four mortality categories, let’s take each in turn. (All graphs for this post by Data Humanist, based on the source data, are free: CC0 (Public Domain)).
Reading the Graphs
In all the four Stabell-Benn, et alia graphs, lower is BETTER: a lower result means lower relative risk versus the placebo for the mRNA vaccines, and lower relative risk versus the placebo/control vaccine for the Adenovirus-vector vaccines.
Overall Mortality
What stands out right away in the graph below: the results for the mRNA vaccine versus the placebo are NOT significant at the 95% Confidence Level. We know this because the Confidence Interval (0.63 to -1.71) crosses the red line at 1. (The estimation itself: 1.03). If you have a relative risk of 1 to 1, or “fifty-fifty” in colloquial English, your risk is the same either way: it makes no difference, vaccine or placebo.
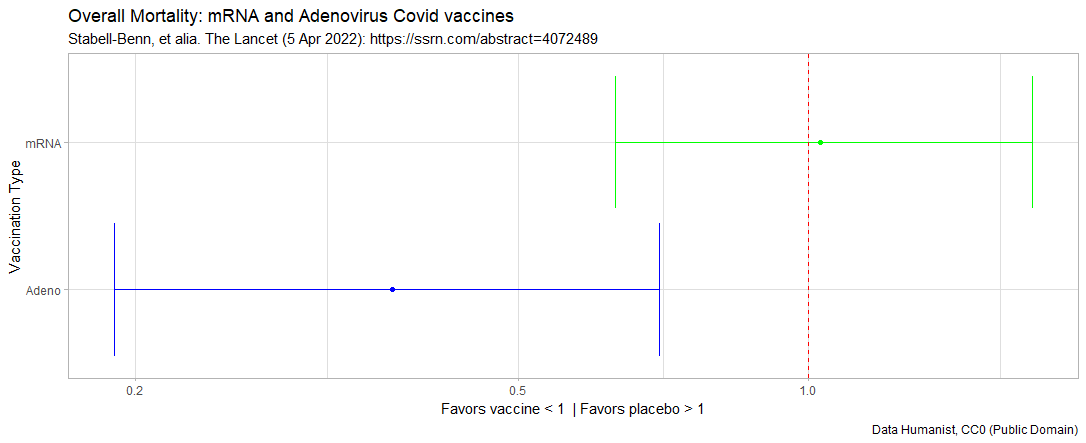
In contrast, versus the placebo/control vaccine, the results for the Adenovirus-vector vaccines are meaningful — statistically significant at the 95% CL. The results are an estimated 0.37 relative risk, in CI of 0.09 to 0.70.
Based upon the data sets studied, the Adeno vaccines DO confer “Beneficial Non-Specific Effects” for Overall Mortality. The mRNA vaccines do NOT — disturbingly, performing no better than the placebo.
If the mRNA vaccines were effective in saving more lives than vaccine complications might take, then shouldn’t the mRNA vaccines also have demonstrated “Beneficial Non-Specific Effects” for Overall Mortality?
Covid-19 Deaths
Surely, both types of vaccines were effective at preventing people from dying from —or, by the American CDC metric, dying with — Covid. Otherwise, what would be point of vaccination? So the data must support this. Only …

Yet again, for the mRNA vaccines we have NO meaningful difference at the 95% CL versus placebo — because in this instance, the relative risk estimation of 0.4 has a CI of 0.08 (quite good) to 2.06 (bad). It trends towards good, but could also be bad: simply too much chance or randomness in the outcome.
In contrast yet again, versus the placebo/control vaccine, the results for the Adenovirus-vector vaccines are meaningful — statistically significant at the 95% CL — with a relative risk estimation of 0.11 in a CI of 0.02 to 0.87. The Adenovirus-vector vaccines unequivocally protect against Covid-19.
Really? Not much of a difference?
So the mRNA vaccines might NOT have made much of a difference in Covid 19 deaths? This might seem at first insane — an impossible result. Understandable.
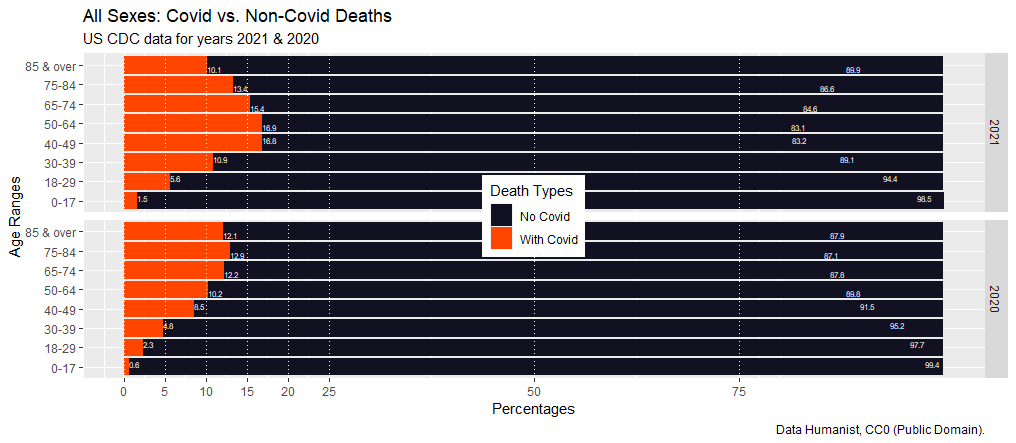
At American Exile, we did an previous (27 January 2022) analysis of the American CDC data “Provisional Death Counts for COVID-19” for the years 2020 and 2021. The the year with vaccines versus the year with no vaccines:
We will take 2020, Covid Year I, as our “control group” in this natural experiment. Remember, in 2020: no vaccines were widely available — and so no vaccine rollouts or mandates. Blue states were not yet completely sold on lockdowns and the like, and Donald Trump was still President. So 2021, Covid Year II, will serve as our treatment group: vaccines, lockdowns, mandates, Anthony Fauci given free reign, and Joseph Biden as our President.
The results detailed in that post, but below two graphs (again, from the CDC’s own data). The first shows the percentages of Deaths with Covid-19 to All Other Deaths; the second shows the Relative Risk ratios by Age Category for 2021 to 2020.
Covid vs. Non-Covid Deaths: Percentages for 2021 vs 2020
For the graph below, the larger the red bar, the greater the share of Deaths with Covid.
Relative Risk of Dying With Covid: 2021 vs. 2020
For the graph below, a higher relative risk of Dying with Covid is NOT good.

We checked and re-checked the data and these results before posting, because the results seemed insane. How could we have more people dying with Covid in 2021, and in five of the seven age categories a higher relative risk, if we had the massive vaccination campaign, the mandates and lockdowns, and so on? But the USA did.
When we published these results back on 27 January 2022, we did so with fear of being denounced, or sued, or whatever — because the results seemed so improbable, despite constantly rechecking the CDC’s own data and the simple math involved in the calculations. Instead, the results were ignored — safety in obscurity!
It also helps that we do not have a Twitter account, and so could not share there. So that post again; and a Data dashboard here, with the CDC data set free for download;.
The CDC data again, similar to Stabell-Benn, et alia, raises doubt about mRNA vaccine efficacy. But let us refer you to two highly qualified scientists.
Martin Kulldorff and Jay Bhattacharya on Stabell-Benn, et alia
In commenting upon Stabell-Benn, et alia, Martin Kulldorf (22 April 2022) had the courage to ask: Have People Been Given the Wrong Vaccine?
Jay Bhattacharya (3 May 2022), following up in part on Kulldorf, calls attention to both the limits (acknowledged by Stabell-Benn, et alia) and the importance of this study comparing the mRNA vaccines to the adenovirus vaccines: Study into mRNA vaccine death rates sends ‘danger signals.’
Since sadly the MSM largely refuses to pay attention to elite scientists who dissent from the Covid Narrative, let nobody us make one more source available in the wilds of Substack for the truly intrepid. Our exploration of Stabell-Benn, et alia, continues.
Cardiovascular Deaths
This brings us to the third vital category of mortality considered by Stabell-Benn, et alia, Cardiovascular Deaths. We know that myocarditis is one possible complication of the vaccines. How do the two vaccine types compare?

Please keep in mind, lower is better as it shows the relative risk. For the mRNA vaccines we have NO meaningful difference at the 95% CL versus placebo. But in this case, the relative risk estimation of 1.45 has a CI of 0.67 to 3.13. So the trend is NOT good, although also not statistically significant at this level: otherwise, it would appear that the mRNA vaccines put people at GREATER risk than the placebo for cardiovascular death. Again, however, not meaningful at a 95% CL.
In contrast versus the placebo/control vaccine, the results for the Adenovirus-vector vaccines are meaningful — statistically significant at the 95% CL — with a relative risk estimation of 0.07 in CI of 0.01 to 0.41. Based on these results, the Adeno vaccines DO confer “Beneficial Non-Specific Effects” which reduce cardiovascular death risk.
Non-Accidental, Non-Covid Deaths
The final category evaluated by Stabell-Benn, et alia, strikes us as too loosely defined to weight strongly. But yet again, we have the same story. For the mRNA vaccines, we have NO meaningful difference versus placebo at the 95% CL: a relative risk estimation of 1.17 in CI of 0.67 to 2.05.

But versus the placebo/control vaccine, the Adenovirus-vector vaccines have meaningful results — statistically significant at the 95% CL — with a relative risk estimation of 0.38 in CI of 0.17 to 0.88.
In all four categories, the mRNA vaccines fail to produce statistically meaningful results that would clearly indicate effectiveness and preferably also “Beneficial Non-Specific Effects.”
Kulldorff’s Harsh But Astute Summaries
In the comments below, Kulldroff (22 April 2022) is referring to overall mortality in the first two bullet points.
There is clear evidence that the adenovirus-vector vaccines reduced mortality.
For the mRNA vaccines, on the other hand, there was no evidence of a mortality reduction.
For the mRNA vaccines, there was a reduction in Covid deaths but an increase in cardiovascular deaths, but neither was statistically significant.
So, either result could be due to random chance.
Alternatively, the vaccines may reduce the risk for Covid deaths while increasing the risk for cardiovascular deaths.
Comments on Kulldorff & on Stabell-Benn, et alia
So did the mRNA vaccines work? First, at reducing the risk of people dying from Covid-19? Second, doing this without causing an equal or greater number of deaths? The cure must not be worse than the disease.
Now going on two years, we lack hard evidence that the mRNA vaccines work as promised; or that even if so, that the mRNA vaccines save more lives than they take.
If the work of Stabell-Benn, et alia, holds up, their findings are damning. Absolutely damning. We had a less expensive, less risky, and more beneficial alternative: the Adenovirus-vector vaccines.
Instead, the FDA, the CDC, and Big Pharma coercively imposed upon the American people — and did their best to impose upon much of the global public — the mRNA vaccines of Pfizer and Moderna. Our power elite still wish to — are still trying to —mRNA vaccinate all the American children.
In Michael Kerr’s Dispatches, perhaps the classic account of the Vietnam War, a young soldier weary from his time at the front lines says: “I hate this movie.” Knowing full well, of course, his experience was not a movie. At American Exile, we hate this current movie — this Sci-Fi dystopia of greedy technocrats operating without constraint on the American public and on much of the global public.
Key Sources
Professor Christine Stabell-Benn discusses her study in the video below (3 May 2022), Danish professor: mRNA vaccine study sends 'danger signals'.
The suggested citation for the Stabell-Benn, et alia study:
Benn, Christine Stabell and Schaltz-Buchholzer, Frederik and Nielsen, Sebastian and Netea, Mihai G. and Netea, Mihai G. and Aaby, Peter, Randomised Clinical Trials of COVID-19 Vaccines: Do Adenovirus-Vector Vaccines Have Beneficial Non-Specific Effects?. Available at SSRN: https://ssrn.com/abstract=4072489 or http://dx.doi.org/10.2139/ssrn.4072489
Thank you sincerely for considering American Exile as an alternative source of analysis and commentary.
Free Graphs: The graphs created by Data Humanist for this post are licensed CC0 (Public Domain), and are free to use however you see fit.
Standard disclaimer: Our link to or citation of any source or person does NOT imply that source or person in anyway endorses American Exile. Our preferred pronouns remain: “small fringe minority” & “unacceptable views.”